Heart disease is killing us – over 34% of deaths in America are preventable.
President Lyndon B. Johnson, a heart attack survivor, issued the first proclamation in 1964 that February is American Heart Month. Since then, the nation has spotlighted heart disease every February, the number one killer of Americans (over 34% of annual deaths) and the leading cause of death globally (1). And since heart disease and cholesterol are practically synonymous with one another, I need to tell you something really important. Cholesterol is the natural band-aid your body makes to repair cardiovascular damage. It’s part of our innate design, but the problem is when it gets out of control. More on that later.
What is Cardiovascular Disease?
Cardiovascular disease (CVD) encompasses a range of conditions: heart attacks, strokes & peripheral arterial disease. It also contributes towards metabolic syndrome, nonalcoholic fatty liver disease, diabetes, chronic kidney disease and COVID mortality. Subsequently, CVD is the leading cause of death for individuals who have diabetes, advanced kidney disease, and non-alcoholic fatty liver disease (2, 3, 4).
Price & Prevention of Cardiovascular Disease
So what are the factors that play into the development of CVD, and most importantly, how do we prevent it?
Before I dive into that, I have been pondering over the question, “What is the cost of a heart attack?” And I do not mean just financially. What is the overall impact to yourself, your family and your friends? What about the way you live the rest of your life as a survivor? What about access to effective cardiac rehabilitation? I work with clients every day to prevent heart disease, but can we really grasp the value of that offering? According to the Agency for Healthcare Research and Quality, the average heart attack patient pays $21,500 per hospital stay out of pocket and some patients end up paying upwards of $100,000 when surgery is involved (5). Dr. Polly Galbraith is the VP and chief medical director of Assurant, an insurance provider. She reports that the lifetime cost of treating a severe heart attack with insurance can reach $1 million and strokes can easily hit $2 million if long-term nursing facilities are needed. Is anyone else no longer wondering why our insurance premiums are so high if about 805,000 people in the United States have a heart attack yearly (6)? We are collectively spending money to remain ill as the majority of education around heart disease is directed at treatment and not prevention.
“It really doesn’t matter if your cholesterol levels are perfect. If you have arterial damage, you are forming plaque.”
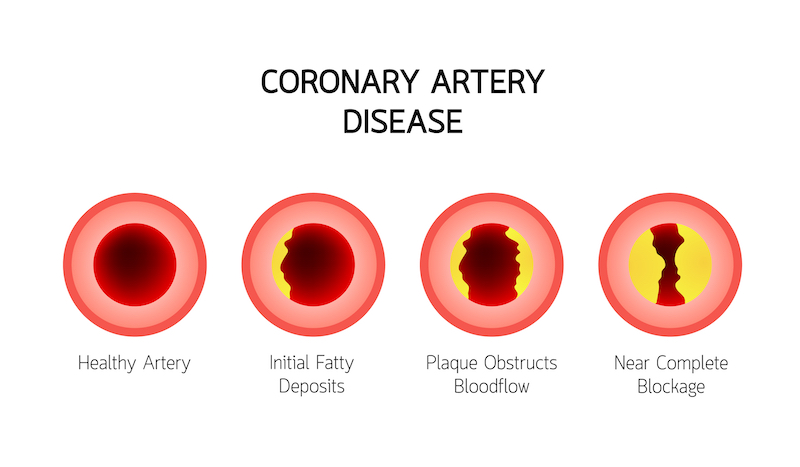
Decreases in overall CVD deaths have been associated with effective primary prevention strategies, such as lifestyle modification, blood pressure control and properly managing cholesterol (7). The factors that play into the development of CVD are hypertension, vascular inflammation, lipid abnormalities, plaque formation, diabetes mellitus, cigarette smoking and sedentary lifestyle. The easiest way to explain the pathophysiology of CVD is that plaque cannot form in arterial walls without some sort of damage happening to the endothelium (lining of the blood vessels) first. This usually occurs from uncontrolled hypertension, genetic abnormalities in repair processes (MTHFR), infections in the teeth or blood, or chemicals in cigarettes. Once the damage is done, your body uses its #1 natural band-aid to cover up the injury: CHOLESTEROL. It really doesn’t matter if your cholesterol levels are perfect. I’ll say that again. It really doesn’t matter if your cholesterol levels are perfect. If you have arterial damage, you are forming plaque. This is why “perfectly healthy people” can drop dead of heart attacks out of the blue. I’ll go more into the markers I run to test for vascular damage and risk later.
Role of Hypertension in Preventing Cardiovascular Disease

Back to prevention: the number 1 move is to get hypertension under control. And just how important is that?
- Per the CDC, nearly 1 in 2 US adults have hypertension, and only 1 in 4 have it under control (8).
- High blood pressure was a primary or contributing cause of death for 516,955 people in the United States in 2019 (9). This is separate and in addition to the CVD statistics mentioned above!!
- High blood pressure costs the United States about $131,000,000,000 (that’s billion) each year, averaged over 12 years from 2003 to 2014 (10).
There are many ways to address hypertension, because hypertension can be caused by many things. If your primary care doctor is just bouncing you from one drug to the next (ACEi, ARB, CCB…) and they haven’t tested your aldosterone levels, run a renal artery ultrasound or spoken with you about changing your diet or stress management – they’re not interested in WHY you have hypertension. I work with my clients to thoroughly understand contributing factors to disease so that we can reverse and even CURE it. Sometimes it’s complex and multifactorial. The urgency is to get blood pressure well controlled so that it does not contribute to CVD and plaque formation. Additionally I’m seeing a lot of new and uncontrollable hypertension post COVID immunization and/or booster. If that feels familiar to you, please speak with your primary care doctor – soon.
Blood Tests: Uncovering Hidden Inflammation
The other major contributors to CVD we can often look for in blood tests. The annual blood panel I run on most of my clients includes cardiovascular inflammation markers (hs-CRP and homocysteine) and a thorough NMR lipid assessment. hs-CRP tells us your risk of developing coronary artery disease, which often leads to a heart attack. Homocysteine gives us a numerical value for vascular damage (the root issue of plaque formation). The advanced lipid panel I run (LipoFraction NMR) through Cleveland Heart Labs, gives us a much more in depth look at all protective and inflammatory lipid markers. I use this to assess what is the actual risk of plaque formation in combination with hs-CRP and homocysteine levels. All of these labs can be requested by your primary care doctor. My clinic runs them all for less than $100 out-of-pocket.
Other Tests for Preventing CVD
Some other tests I would like to make you all aware of that most clients should consider beginning in their 40’s or 50’s, depending on family history: Carotid Ultrasound and Coronary Artery Calcium Score. Both are very non-invasive imaging done to assess soft plaque formation (Carotid US) and hard plaque formation (Coronary Artery Calcium). Nevada imaging centers will charge around $200 out-of-pocket for both, and many doctors will refer you for these with insurance coverage. If you have had elevated homocysteine and lipid levels for a long period of time, I highly recommend assessing “the damage that has been done” with one or both of these tests. The good news is that plaque formation is entirely reversible addressing the root causes of why it has happened. I attack this with proper nutrition, exercise and supplements that can break down and metabolize the plaques. It takes work, but it’s a lot less work than a heart attack.
Recap: Preventing Cardiovascular Disease
I am a doctor, but I may not be your doctor. Some take home points:
- Ask for appropriate labs to assess cardiovascular risk: hs-CRP, homocysteine, & LipoFraction NMR
- Get contributing factors for CVD under control: hypertension, vascular inflammation, lipid abnormalities, plaque formation, diabetes mellitus, cigarette smoking and sedentary lifestyle
- If needed, get imaging to assess advancing plaque formation: Carotid Ultrasound and/or Coronary Artery Calcium Score

Other things I find helpful are high-dose bioflavonoids or anthocyanins, which are commonly found in deeply pigmented berries and fruits. I’ve seen multiple clients waiting for stents or arterial blockages to be removed start on high-dose anthocyanins, and months later be turned away for the procedure because it was no longer necessary. The benefits of these bioflavonoids are countless: reducing cardiovascular incidents, reversing arterial disease, helping with diabetes and even reversing macular degeneration. We do an annual sale of this product every February: Fruit Anthocyanins by Dr. Bill Mitchell. If you are interested in purchasing, please contact us at in**@na************.com. 1 tsp of the syrup has the antioxidant equivalent of an entire pint of organic berries. You can read more about the benefits here: Letter from Dr. Bill Mitchell & Research Summary.
Take Ownership of Your Health
I have been thinking about writing this piece for months. Most clients come to me with a specific issue: IBS, depression, hypertension, etc. While I’m working with them on what is most important to them at the moment, I’m always thinking of how to get them to 75 years old without a heart attack and to 90 without a hip fracture. If you’re a client of mine – you’ve heard me say this to you. This is why having someone on your team who is interested in prevention is critical to your long-term health. I catch elevated hs-CRP in 30 year olds and elevated homocysteine in 14 year olds. Addressing those issues at those ages kicks out that first heart attack by a decade – or maybe it will never happen at all. We need to be more aggressive when it comes to cardiovascular disease prevention. It’s been the leading cause of death in the US since 1921 (11). That’s over 100 years!!! And we don’t have much to show for it nationally – so let’s take ownership of our health and start asking for preventative measures from our healthcare providers.
Footnotes
(1) Cardiovascular diseases. World Health Organization. Accessed August 8, 2021. https://www.who.int/health-topics/cardiovascular-diseases#tab=tab_1
(2) Schmidt AM. Diabetes mellitus and cardiovascular disease. Arterioscler Thromb Vasc Biol. 2019;39(4):558-568. doi:10.1161/ATVBAHA.119.310961
(3) Jankowski J, Floege J, Fliser D, et al. Cardiovascular disease in chronic kidney disease: pathophysiological insights and therapeutic options. Circulation. 2021;143(11):1157-1172. doi:10.1161/CIRCULATIONAHA.120.050686
(4) Mitra S, De A, Chowdhury A. Epidemiology of non-alcoholic and alcoholic fatty liver diseases. Transl Gastroenterol Hepatol. 2020;5:16. doi:10.21037/tgh.2019.09.08
(5) Agency for Healthcare Research and Quality (AHRQ).Cardiovascular/Cerebrovascular Conditions and Procedures 2001 to 2012. U.S. Department of Health and Human Services. Retrieved 16 September 2021 from https://www.hcup-us.ahrq.gov/reports/projections/2012-02.pdf
(6) Fryar CD, Chen T-C, Li X. Prevalence of uncontrolled risk factors for cardiovascular disease: United States, 1999–2010 pdf icon[PDF-494K]✎ EditSign. NCHS data brief, no. 103. Hyattsville, MD: National Center for Health Statistics; 2012. Accessed May 9, 2019.
(7) Mechanick JI, Farkouh ME, Newman JD, et al. Cardiometabolic-based chronic disease, adiposity and dysglycemia drivers: JACC State-of-the-Art Review. J Am Coll Cardiol. 2020;75(5):525-538. doi:10.1016/j.jacc.2019.11.044
(8) Centers for Disease Control and Prevention. Hypertension Cascade: Hypertension Prevalence, Treatment and Control Estimates Among U.S. Adults Aged 18 Years and Older Applying the Criteria from the American College of Cardiology and American Heart Association’s 2017 Hypertension Guideline—NHANES 2015–2018external icon. Atlanta, GA: U.S. Department of Health and Human Services; 2021. Accessed March 12, 2021.
(9) Centers for Disease Control and Prevention, National Center for Health Statistics. About Multiple Cause of Death, 1999–2019. CDC WONDER Online Database website. Atlanta, GA: Centers for Disease Control and Prevention; 2019. Accessed February 1, 2021. (10) Centers for Disease Control and Prevention. Hypertension Cascade: Hypertension Prevalence, Treatment and Control Estimates Among U.S. Adults Aged 18 Years and Older Applying the Criteria from the American College of Cardiology and American Heart Association’s 2017 Hypertension Guideline—NHANES 2015–2018external icon. Atlanta, GA: U.S. Department of Health and Human Services; 2021. Accessed March 12, 2021. (11) https://www.cdc.gov/mmwr/preview/mmwrhtml/mm4830a1.htm#:~:text=Heart%20disease%20has%20been%20the,approximately%2040%25%20of%20all%20deaths.

I want to subscribe to your blog.